
Modelling the projected clinical and Environmental burden of CKD in Egypt and Morocco between 2025 and 2030
This poster, presented at the World Congress of Nephrology 28–31 March 2026 presents work on the clinical and environmental burden of chronic kidney disease (CKD) in Egypt and Morocco between 2025 and 2030. Virtual populations representative of Egypt and Morocco were generated using a microsimulation model. Modelled individuals progressed through CKD stages based on age-related estimated glomerular filtration rate (eGFR) decline rates, and associated comorbidities. Between 2025 and 2030, CKD prevalence was projected to increase substantially in both countries from 5.58m to 7.72m cases in Egypt and from 1.58m to 1.86m in Morocco, with a corresponding significant increase in the environmental impact arising from heamodialysis. Potential responses to mitigate this burden include the implementation of national and regional strategies for early CKD screening and treatment, and integrated approaches to environmental sustainability to mitigate the projected clinical and environmental burden of CKD.
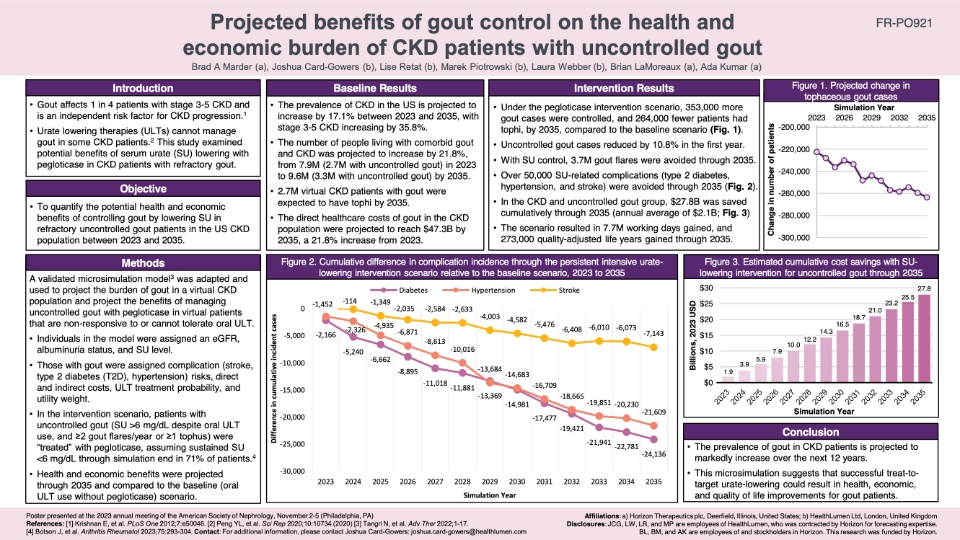
Projected benefits of gout control on the health and economic burden of CKD patients with uncontrolled gout
This poster, presented at the annual meeting of the American Society of Nephrology in Philadelphia, USA (November, 2023) outlines the findings of a study examining the potential benefits of serum urate (SU) lowering using pegloticase in chronic kidney disease (CKD) patients with refractory gout. The study, using microsimulation modelling, found that under a pegloticase intervention scenario, 353,000 more gout cases were controlled, and 264,000 fewer patients had tophi, by 2035, compared to the baseline scenario. Further, the SU lowering intervention was projected to save $27.8B, and gain 7.7M working days, cumulatively through 2035. This study consequently provides evidence that successful treat-to-target urate-lowering could result in health, economic, and quality of life improvements for gout patients.

Inside CKD: Projecting the Population Level Clinical Burden of Chronic Kidney Disease According to Urine Albumin-to-Creatine Ratio (uACR) Categories
This study assessed the future epidemiological and financial burden of CKD using the Inside CKD microsimulation. Specifically, it reports on the CKD population level projections for cardio-renal complications, progression to end stage kidney disease (ESKD), and death due to any cause according to uACR categories.
The results support early intervention in the total CKD population, including individuals with normo- or micro-albuminuria, to reduce cardio-renal outcomes, delay progression to ESKD, and therefore avoid the requirement for costly interventions, including heart related hospitalisations, transplantation and dialysis.
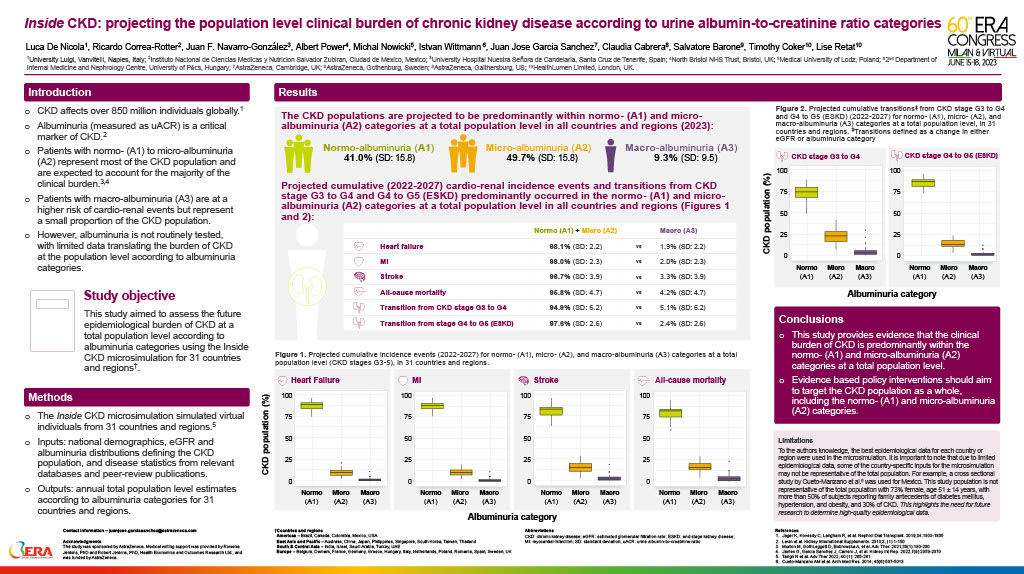
Inside CKD: projecting the population level clinical burden of chronic kidney disease according to urine albumin-to-creatinine ratio categories
This poster, presented at the European Renal Association’s 60th Congress in Milan (June 2023), summarises research on projecting the population level clinical burden of Chronic Kidney Disease (CKD) according to urine albumin-to-creatinine ratio categories. The study provides evidence that the clinical burden of CKD is predominantly within the normo-(A1) and micro-albuminuria (A2) categories at a total population level. Evidence based policy interventions should aim to target the CKD population as a whole, including the normo-(A1) and micro-albuminuria (A2) categories.
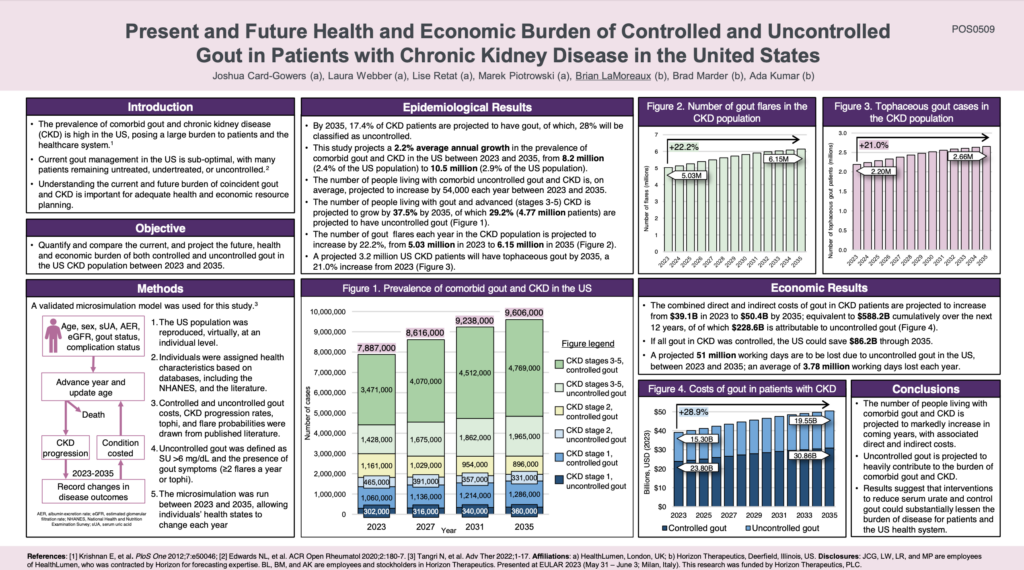
The Present and Future Health and Economic Burden of Controlled and Uncontrolled Gout in Patients with CKD in the US
This poster, presented at EULAR 2023, showcases our new research that projects the increasing health and economic burden of comorbid gout and CKD, in the US, between 2023 and 2035. This study is the first to project the burden of comorbid gout and CKD and highlights the need for strategies that can effectively control gout in CKD patients.
Inside CKD: projecting the economic burden of chronic kidney disease using patient-level microsimulation modelling
As part of the ongoing collaboration between HealthLumen and AstraZeneca to quantify the health and economic burden of Chronic Kidney Disease (CKD), this poster, presented at ISPOR 2021, demonstrates that the burden of CKD is projected to increase by 2026 for all 11 countries included in this analysis. This highlights the need for national policies aimed at early intervention to slow disease progression and reduce healthcare costs.
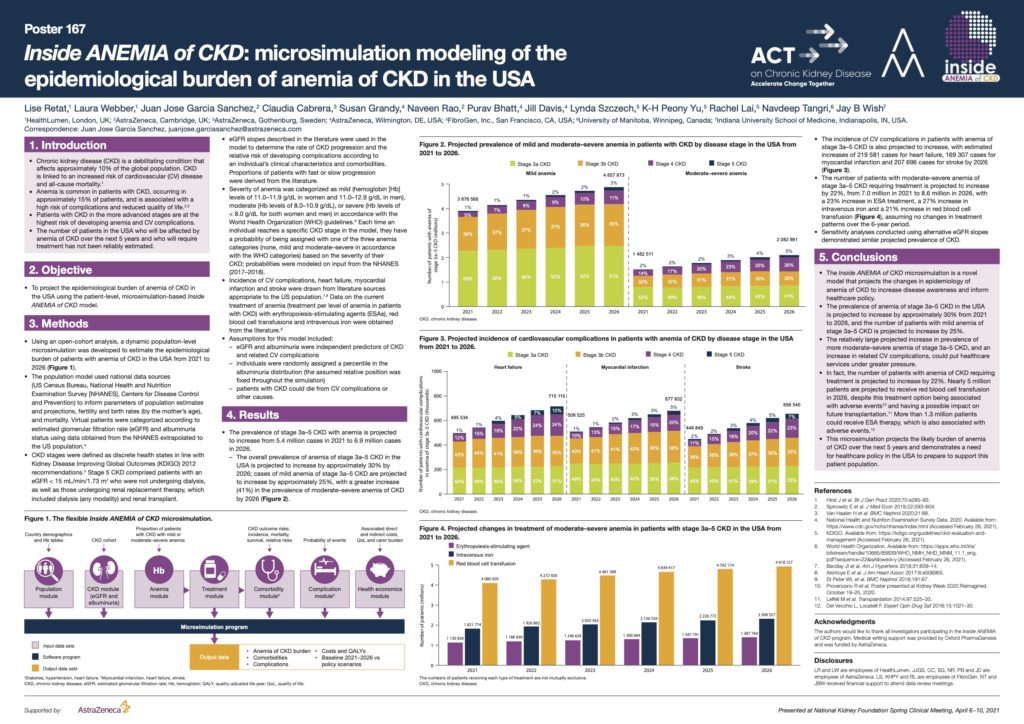
Quantifying the epidemiological burden of anemia of CKD in the USA and Canada via microsimulation modelling
Chronic kidney disease (CKD) is a debilitating condition that affects approximately 10% of the global population. Anemia is common in patients with CKD, occurring in approximately 15% of patients, and is associated with a high risk of complications and reduced quality of life.
The number of patients in the USA and Canada who will be affected by anemia of CKD over the next 5 years and who will require treatment has not been reliably estimated. This study, commissioned by AstraZeneca, projects the epidemiological burden of anemia of CKD in the USA and Canada using a patient-level, microsimulation-model.
In the USA the prevalence of stage 3a–5 CKD with anemia is projected to increase from 5.4 million cases in 2021 to 6.9 million cases in 2026. In Canada, the prevalence of anemia of stage 3a–5 CKD is projected to increase from approximately 1.5 million patients in 2021 to 2.2 million patients in 2026.
The projected increasing prevalence of advanced CKD and associated anemia, as well as the estimated increases in numbers of related cardiovascular (CV) events and patients who will require treatment, could put healthcare systems under greater pressure, and demonstrates a need for healthcare policy in the USA and Canada to prepare to support this patient population.
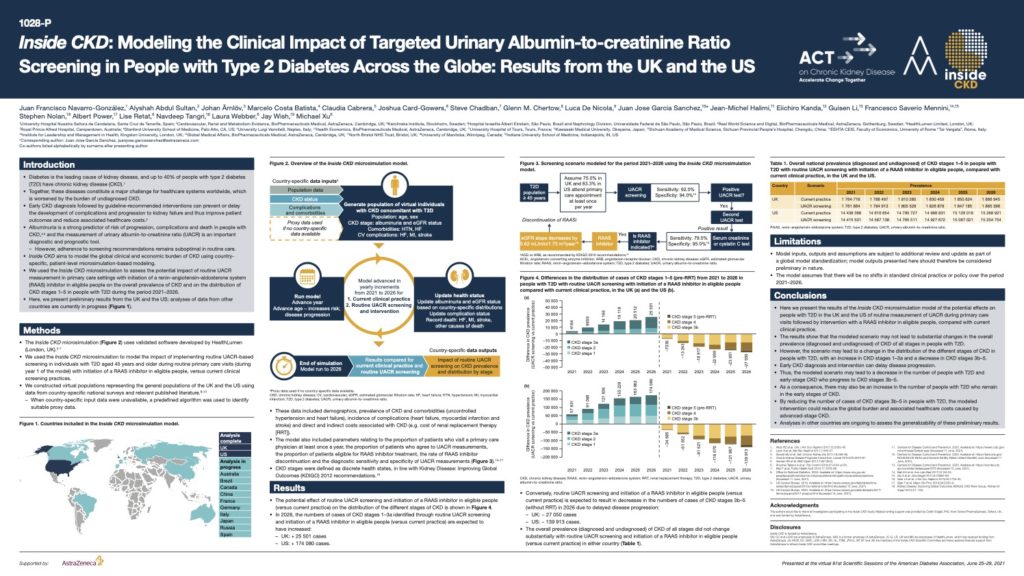
Inside CKD: Modelling the Clinical Impact of Targeted Urinary Albumin-to-creatinine Ratio Screening in People with Type 2 Diabetes Across the Globe
Diabetes is the leading cause of kidney disease, and up to 40% of people with type 2 diabetes (T2D) have chronic kidney disease (CKD) Together, these diseases constitute a major challenge for healthcare systems worldwide, which is worsened by the burden of undiagnosed CKD. Early CKD diagnosis followed by guideline-recommended interventions can prevent or delay the development of complications and progression to kidney failure and thus improve patient outcomes and reduce associated healthcare costs.
Albuminuria is a strong predictor of risk of progression, complications and death in people with CKD and the measurement of urinary albumin-to-creatinine ratio (UACR) is an important diagnostic and prognostic tool.
This poster, presented at the virtual American Diabetes Association’s 81st Scientific Sessions, June 25–29, 2021 demonstrates the potential effects on people with T2D in the UK and the US of routine measurement of UACR during primary care visits followed by intervention with a RAAS inhibitor in eligible people, compared with current clinical practice. By reducing the number of cases of CKD stages 3b–5 in people with T2D, the modelled intervention could reduce the global burden and associated healthcare costs caused by advanced-stage CKD.
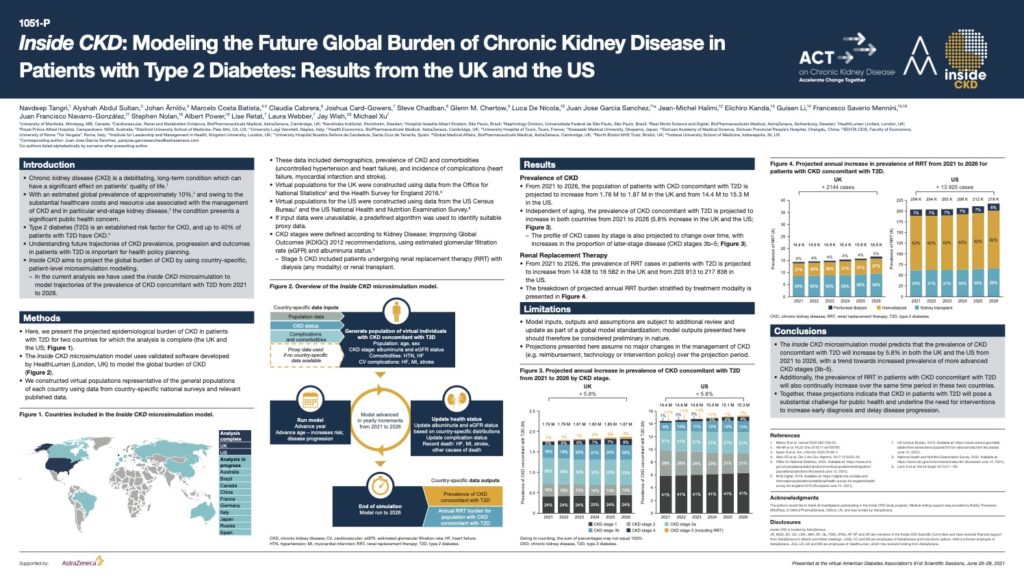
Inside CKD: Modelling the Future Global Burden of Chronic Kidney Disease in Patients with Type 2 Diabetes
Type 2 diabetes (T2D) is an established risk factor for CKD, and up to 40% of patients with T2D have CKD.
This poster, presented at the virtual American Diabetes Association’s 81st Scientific Sessions, June 25–29, 2021 demonstrates that from 2021 to 2026, the population of patients with CKD concomitant with T2D is projected to increase from 1.76 M to 1.87 M in the UK and from 14.4 M to 15.3 M in the US.
These projections indicate that CKD in patients with T2D will pose a substantial challenge to public health and underline the need for interventions to increase early diagnosis and delay disease progression.
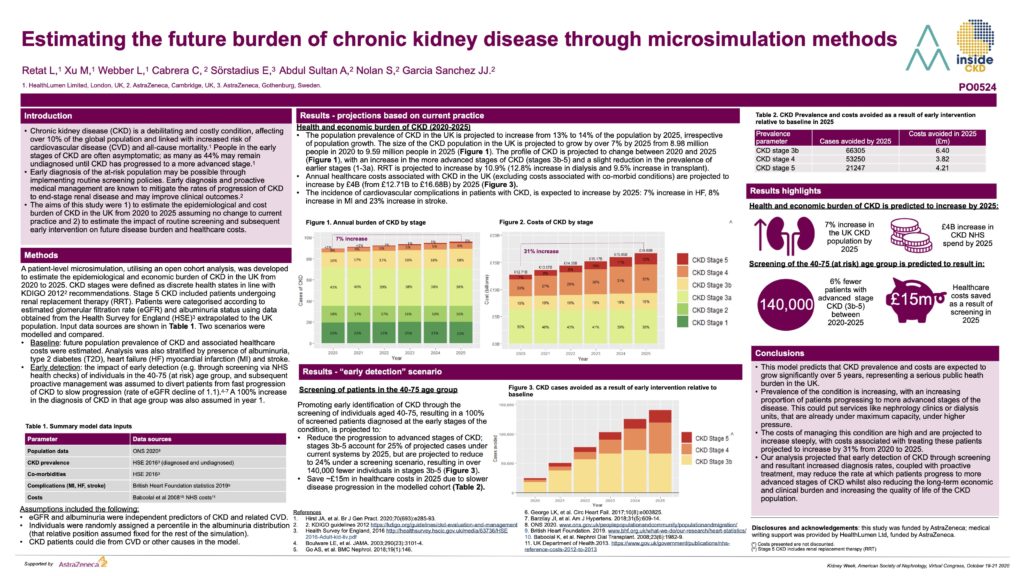
Estimating the future burden of chronic kidney disease through microsimulation methods
Chronic kidney disease (CKD) is a debilitating and costly condition, affecting over 10% of the global population and linked with increased risk of cardiovascular disease (CVD) and all-cause mortality. People in the early stages of CKD are often asymptomatic; as many as 44% may remain undiagnosed until CKD has progressed to a more advanced stage. Early diagnosis of the at-risk population may be possible through implementing routine screening policies. Early diagnosis and proactive medical management are known to mitigate the rates of progression of CKD to end-stage renal disease and may improve clinical outcomes. The aims of this study were 1) to estimate the epidemiological and cost burden of CKD in the UK from 2020 to 2025 assuming no change to current practice and 2) to estimate the impact of routine screening and subsequent early intervention on future disease burden and healthcare costs. Undertaken in partnership with AstraZeneca, this study is now being rolled out to over 20 countries.